




Judit Simon, MD, BA, BSc, Msc, DPhil,FFPH
Professor of Health Economics/Head of Department/Deputy Head of Center
Department of Health Economics, Center for Public Health,
Medical University of Vienna, Austria
Member, ASPHER COVID-19 Task Force
By early afternoon on the 11 November 2020, when this report on the COVID-19 pandemic in Austria is getting finalized, Austria has carried out 2,537,179 COVID-19 tests, registered 172,380 confirmed cases and 1564 COVID-19 related deaths, 3719 patients are hospitalized with 536 cases in intensive care (Figure 1). We are after a very turbulent early November. In the international context, with a backdrop of the most controversial developments in the recent US elections, we just had news of the first effective COVID-19 vaccine, Obamacare (the Affordable Care Act) is challenged again in front of the US Supreme Court, the highest ever COVID-19 infection numbers are being reported in many countries, while Belgian doctors who tested positive for COVID-19 without major symptoms are called to work to tackle hospital staff shortage. At the other end of the COVID-19 pandemic spectrum, Australia recently recorded a few days with no new local COVID-19 cases. More and more European countries including neighboring countries such as Germany, Italy, Slovenia, some of the Swiss cantons, and most recently Hungary have been initiating so called ‘wave breaking’ lockdowns at different levels trying to tackle the second wave of the pandemic. Slovakia has also just completed its mass screening strategy with its impact still to be seen.
Figure 1: COVID-19 Status Quo in Austria (11.11.2020)

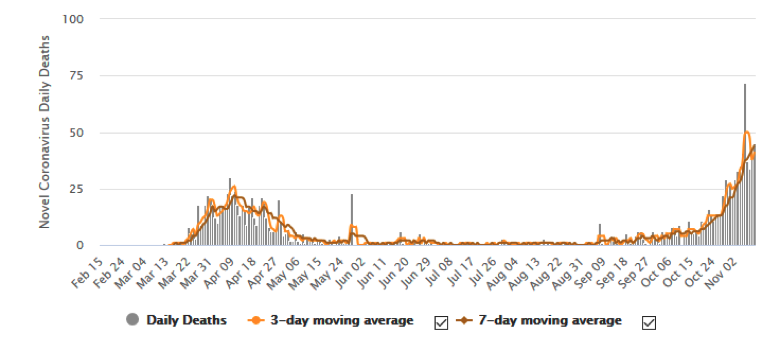
Austria is in lockdown since the 3 November, the same night when a terrible terror attack happened in Vienna. Therefore, the first day of the public health lockdown was spent in the capital city by many (adults and children) at home in an unprecedented ‘terror lockdown’. Since 5 November, all nine Austrian states have been red in the national Corona Traffic Light System (‘Corona Ampel’), a system that was introduced in September for potential regional differentiation of the necessary public health measures and has been reset weekly by a dedicated expert committee since. Austria also registered its highest ever daily COVID-19 cases on the 7 November (8,241 cases, Figure 2) and the highest ever daily COVID-19 deaths on the 6 November (72 deaths, Figure 3).
Figure 2: Daily New Cases in Austria (11.11.2020)
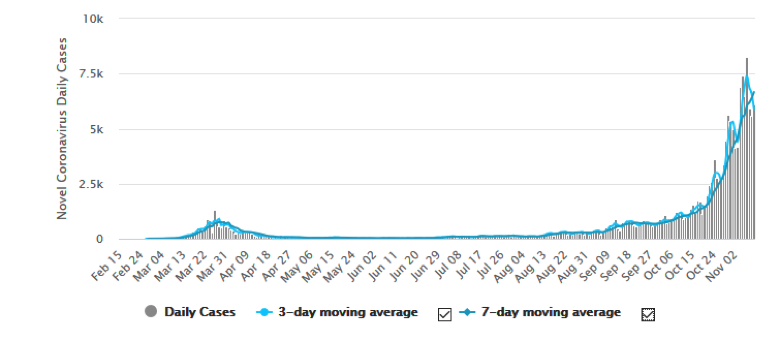
Figure 3: Daily New Deaths in Austria (11.11.2020)
Source: https://www.worldometers.info/coronavirus/country/austria/ (11.11.2020)
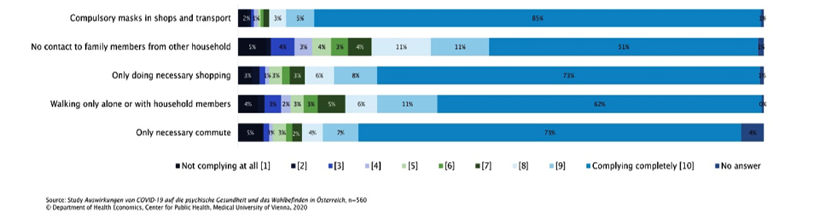
Austria registered its first SARS-Cov2 infection on 25 February 2020. The epicenter of the outbreak was in Ischgl in Tyrol, an internationally well-known and popular ski town. As opposed to the publicly criticized and legally scrutinized delay in regional public health measures which eventually put Ischgl and Sankt Anton under quarantine on the 13 March, Austria had a fairly quick national-level public health response to the COVID-19 outbreak. Firstly, wide-ranging travel restrictions were imposed and border controls were implemented. One of the first measures taken was the prohibition of large public events of over 100 people indoors and over 500 people outdoors on 11 March. Between 16 March and 14 April, the country went into its first national lockdown which included a general prohibition to enter public spaces including leaving homes unless for one of the five exceptions: immediate danger, going to work, shopping for essential goods, caring for others, or exercise outdoors. A distance of 1m was to be kept between all who were not from the same household. Only essential shops remained open. In order to limit gatherings even further, universities and schools were closed and switched to distant learning. Home office arrangements were requested where and when feasible with relevant temporary social insurance arrangements in place. Doctor’s offices were turned to only receive emergencies, e-prescriptions and medical certificates were provided following telephone consultation. Visitations in hospitals and care homes were also prohibited. On April 6, the Austrian government imposed obligatory mask use in supermarkets. Little over a week later, this was extended to public transport and other small shops which were reopened at that time. The first results of a survey study conducted by the Department of Health Economics, Center for Public Health, Medical University of Vienna show that between 52-75% of the respondents found the public health measures necessary to a certain degree and only 7-17% completely unnecessary. Compliance with the measures was also high, with self-reported rates ranging from 85% considering mask wearing to 51% regarding no contact to family members who live in another household (Figure 4). The same study also found people with a history of mental health treatment as the most negatively impacted vulnerable group by the measures.
Figure 4: Compliance with lockdown measures in Austria, March-April 2020
The spring lockdown was successful in flattening and eventually changing the epidemic curve after about two weeks and allowed the gradual reopening of shops, schools, restaurants from mid April onwards over May (Figure 2). Overall, Austria stood out as a nation that adopted aggressive and early control strategies and thereby saw a much smaller proportion of deaths from COVID-19 in the first wave compared to some other European countries.
After a summer with fairly low case numbers and life seemingly returning to post-COVID normality (e.g. mask wearing compulsory in public transport and in some essential shops, possibility for ongoing home office arrangements, mask wearing compulsory in common areas of schools), first concerns about a second wave of the pandemic surfaced by September with very rapid increase in case numbers since. We are now in a second national COVID-19 lockdown in Austria. While all recreational, culture and indoor sport facilities had to close similar to the situation in spring, some public health measures are different this time. All shops remained open with max. 1 person per 10m2 allowed. There is a night curfew between 8pm and 6am with an obligatory closing time at 7pm. In the gastronomy, only delivery or pick-up is allowed. Hotels can receive only business clients. Everywhere minimum 1 m distance between persons is to be kept together with compulsory mask wearing in all public indoor places and public transport. Events in general are prohibited, except professional sport events without spectators and funerals with max. 50 persons. Hobby sport is only allowed outdoors where all the distancing and hygienic measures can be adhered to (no contact or team sport). Care home visits are possible, but with major restrictions. Home office is recommended where feasible, but not compulsory. Teaching from 14 years onward and in universities are all online, but schools for younger children and kindergartens remained open as per a different ‘Corona Ampel for Education’ which is kept at orange level for the time being. This latter decision is also supported by the cluster analysis of AGES (Austrian Agency for Health and Food Safety) which shows that towards the end of October 52.6% of the cases were contracted in private households, 22.6% in recreational settings, 9.2% in health and social care facilities, and only 5.6% in educational settings.
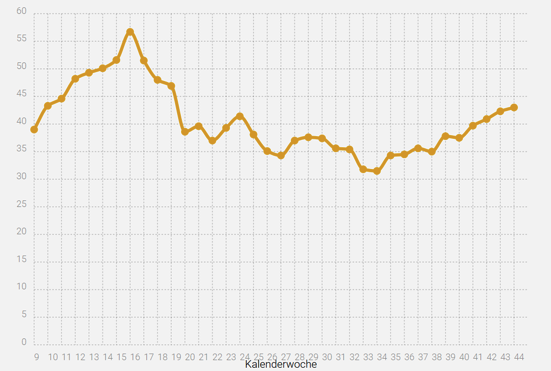
Also the age distribution of the cases seem to differ between now and back in spring. While in April the average age peaked between 55-60 years, in August it was at its so far lowest between 30-35 years with a constant upward trend since to the current average age of 40-45 years. (Figure 5)
Figure 5: Average age of confirmed COVID-19 cases per calendar week in 2020 (11.11.2020)
Source: https://www.ages.at/en/topics/pathogenic-organism/coronavirus/
Testing in Austria has been mostly based on the gold standard PCR-test with 281,127 test per 1 million population carried out so far with active contact tracing in place from early on. Currently a free test may be done at home, in school or work following a suspected case or close contact reported to the health authorities via the 1450 hotline, via compulsory weekly testing for employees in health care and social care facilities, optional testing in educational facilities, and upon own initiative via drive-in facilities. According to recent news, however, the follow-up of contacts is now only feasible for approximately 1:4 cases due to the exponentially increased case numbers with an R of 1.33 as the beginning of November. To allow faster and easier sample taking, a so called ‘gargel test’ (Gurgeltest) delivered by mobile bicycle carriers was introduced on 21 September for educational facilities. Recent analysis of these test results revealed an overall 3.52% positivity. To address the upcoming flu season, special container units will also start operating for the screening of self-registered symptomatic patients using the less precise but faster and cheaper antigen tests with an attempt to support fast differential diagnosis of respiratory infectious cases and keep these out of main health care facilities from tomorrow onwards.
The Austrian government’s employment support policy implemented in the early stages of the pandemic included the introduction of a short-term working scheme to help retain jobs. While in ‘Kurzarbeit’, employees received 80% of their salary financed by the government allowing employers to retain staff. Businesses could also apply for direct financial support and tax relief. Despite these measures, the unemployment rate in Austria increased from 8.1% in February to 12.7% in April and eventually reduced back to 8.4% by September. During the recent lockdown, hotels and service providers required to close will be compensated with 80% of their turnover based on the same period from last year. In October only a slight increase in the unemployment rate to 8.7% could be observed (https://www.statista.com/statistics/1116338/unemployment-rate-by-month-austria/). In order to ‘save’ winter tourism and winter sports, all gondolas and lifts will also be closed for the time of the current lockdown and even if a reopening will become feasible in December, apres ski will be prohibited during the forthcoming winter season. In any case, the legal basis for home office arrangements is still missing in Austria and is not expected to be provided before early 2021 leaving a major grey area for all employers and employees under the current circumstances.
Regarding resources, although Austria has the second highest number of doctors and fifth highest number of hospital beds in the OECD relative to its population (5.2 practising doctors and 7.4 hospital beds per 1 000 people, OECD Health at a Glance 2019) and, therefore, is expected to be one of the most resilient European health care systems in terms of shortage of hospital beds or staff, recent predictions warn about intensive care capacity shortages already in November if the current lockdown measures do not work. Some regions, for example, Carinthia, have already indicated the highest level of hospital capacity usage and started postponing non-emergency care. There are also speculations about further national-level restrictive measures being implemented over the next few days. What the direct pandemic impact of the recent public health measures are, however, will only be evident in about another week, its long-term consequences only in the years to come.
Further information: